

DeQuervain's syndrome
Encyclopedia
De Quervain syndrome is a tendinosis
of the sheath or tunnel that surrounds two tendon
s that control movement of the thumb
.
surgeon
Fritz de Quervain
who first identified it in 1895. It should not be confused with de Quervain's thyroiditis
, another condition named for the same person.
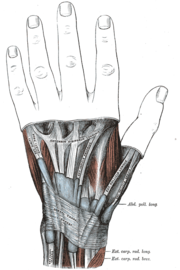 The two tendons concerned are the tendons of the extensor pollicis brevis and abductor pollicis longus muscles. These two muscles, which run side by side, have almost the same function: the movement of the thumb away from the hand in the plane of the hand—so called radial abduction (as opposed to movement of the thumb away from the hand, out of the plane of the hand (palmar abduction)). The tendons run, as do all of the tendons passing the wrist, in synovial sheath
The two tendons concerned are the tendons of the extensor pollicis brevis and abductor pollicis longus muscles. These two muscles, which run side by side, have almost the same function: the movement of the thumb away from the hand in the plane of the hand—so called radial abduction (as opposed to movement of the thumb away from the hand, out of the plane of the hand (palmar abduction)). The tendons run, as do all of the tendons passing the wrist, in synovial sheath
s, which contain them and allow them to exercise their function whatever the position of the wrist. Evaluation of histological specimens shows a thickening and myxoid degeneration consistent with a chronic degenerative process. The pathology is identical in de Quervain seen in new mothers.
De Quervain's is more common in women; the speculative rationale for this is that women have a greater angle of the styloid process
of the radius.
.
Some claim that this diagnosis should be included among overuse injuries
and that repetitive movements of the thumb are a contributing factor, but there are no scientific data that support a link between hand use and de Quervain's.
Finkelstein's test
is used to diagnose de Quervain syndrome in people who have wrist pain. To perform the test, the examining physician grasps the thumb and the hand is ulnar deviated sharply, as shown in the image. If sharp pain occurs along the distal radius (top of forearm, about an in inch below the wrist; see image), DeQuervain's syndrome is likely.
Differential diagnosis includes ruling out:
Retrospective studies all report success rates for corticosteroid injection greater than 70%, but the one prospective cohort study noted a success rate of only 58% and many of those patients took 12 to 18 months until symptom resolution. While the authors of that study ascribed the failure of corticosteroid injection to anatomical variations, it has not been clearly established that corticosteroid injection is better than placebo or that a symptom course of 12 to 18 months is any better than the natural course of the illness.
Another commonly used criterion for failure of non-operative treatment is election of operative treatment, but the decision to operate is complex and biased by the beliefs and emotions of the surgeon and the patient. Use of an elective event such as surgery to define success makes data regarding nonoperative treatment difficult to interpret. For instance, in one of the two investigations in which a substantial number of patients were treated without injection (splints and anti-inflammatory medication alone were used), a remarkable 45 of 93 (48%) of patients in all non-operative treatment groups had surgery. This may simply reflect frustration on the part of both the patient and the surgeon with the prolonged symptom course associated with the disease. It may appear to both patient and surgeon that, after many months of symptoms, the illness will never resolve. The data of Lane and colleagues indicating that non-operative treatment is successful only in mild cases is similarly marred by the lack of patients randomly assigned to alternative treatments and the use in many patients of a decision for surgery as a failure criterion.
Most tendinoses are self-limiting and the same is likely to be true of de Quervain's although further study is needed. One retrospective series documented resolution in 90% of patients within 1 year
Palliative treatments include a splint that immobilized the wrist and the thumb to the interphalangeal joint and anti-inflammatory medication or acetaminophen.
Surgery (in which the sheath of the first dorsal compartment is opened longitudinally) is documented to provide relief in most patients. The most important risk is to the radial sensory nerve.
Physical/Occupational Therapy often focuses on lifting mechanics even though there is no evidence that activity modification can alter the course of the illness. Therapists can help fashion a splint that provides relief of symptoms by immobilizing the wrist and thumb. Splints have not been demonstrated to change the course of the illness.
Tendinosis
Tendinosis, sometimes called chronic tendinitis, tendinosus, chronic tendinopathy or chronic tendon injury, is damage to a tendon at a cellular level . It is thought to be caused by microtears in the connective tissue in and around the tendon, leading to an increase in tendon repair cells...
of the sheath or tunnel that surrounds two tendon
Tendon
A tendon is a tough band of fibrous connective tissue that usually connects muscle to bone and is capable of withstanding tension. Tendons are similar to ligaments and fasciae as they are all made of collagen except that ligaments join one bone to another bone, and fasciae connect muscles to other...
s that control movement of the thumb
Thumb
The thumb is the first digit of the hand. When a person is standing in the medical anatomical position , the thumb is the lateral-most digit...
.
Eponym
It is named after the SwissSwitzerland
Switzerland name of one of the Swiss cantons. ; ; ; or ), in its full name the Swiss Confederation , is a federal republic consisting of 26 cantons, with Bern as the seat of the federal authorities. The country is situated in Western Europe,Or Central Europe depending on the definition....
surgeon
Surgery
Surgery is an ancient medical specialty that uses operative manual and instrumental techniques on a patient to investigate and/or treat a pathological condition such as disease or injury, or to help improve bodily function or appearance.An act of performing surgery may be called a surgical...
Fritz de Quervain
Fritz de Quervain
Fritz de Quervain was a Swiss surgeon born in Sion. He was a leading authority on thyroid disease.In 1892 he received his doctorate from the University of Bern, and several years later became director of the surgical department at a hospital in La Chaux-de-Fonds in the canton of Neuchâtel...
who first identified it in 1895. It should not be confused with de Quervain's thyroiditis
De Quervain's thyroiditis
de Quervain's thyroiditis, can also be known as subacute granulomatous thyroiditis or Giant Cell Thyroiditis. Males and females of all ages are affected...
, another condition named for the same person.
Pathology
Synovial sheath
A synovial sheath is a layer of a tendon sheath containing tendons in the hand and foot.They lie internal to the fibrous tendon sheaths.An example is the common synovial sheath for the flexor tendons....
s, which contain them and allow them to exercise their function whatever the position of the wrist. Evaluation of histological specimens shows a thickening and myxoid degeneration consistent with a chronic degenerative process. The pathology is identical in de Quervain seen in new mothers.
De Quervain's is more common in women; the speculative rationale for this is that women have a greater angle of the styloid process
Styloid process
In anatomy, a styloid process , usually serving as points of attachment for muscles, refers to the slender, pointed process of :* temporal bone of the skull - Temporal styloid process...
of the radius.
Cause
The cause of de Quervain's disease is not known. In medical terms, it remains idiopathicIdiopathic
Idiopathic is an adjective used primarily in medicine meaning arising spontaneously or from an obscure or unknown cause. From Greek ἴδιος, idios + πάθος, pathos , it means approximately "a disease of its own kind". It is technically a term from nosology, the classification of disease...
.
Some claim that this diagnosis should be included among overuse injuries
Repetitive strain injury
Repetitive strain injury is an injury of the musculoskeletal and nervous systems that may be caused by...
and that repetitive movements of the thumb are a contributing factor, but there are no scientific data that support a link between hand use and de Quervain's.
Symptoms
Symptoms are pain, tenderness, and swelling over the thumb side of the wrist, and difficulty gripping.Finkelstein's test
Finkelstein's test
Finkelstein's test is used to diagnose DeQuervain's tenosynovitis in people who have wrist pain. To perform the test, the examining physician grasps the thumb and the hand is ulnar deviated sharply, as shown in the image...
is used to diagnose de Quervain syndrome in people who have wrist pain. To perform the test, the examining physician grasps the thumb and the hand is ulnar deviated sharply, as shown in the image. If sharp pain occurs along the distal radius (top of forearm, about an in inch below the wrist; see image), DeQuervain's syndrome is likely.
Differential diagnosis includes ruling out:
- OsteoarthritisOsteoarthritisOsteoarthritis also known as degenerative arthritis or degenerative joint disease, is a group of mechanical abnormalities involving degradation of joints, including articular cartilage and subchondral bone. Symptoms may include joint pain, tenderness, stiffness, locking, and sometimes an effusion...
of the first carpo-metacarpal joint - Intersection syndromeIntersection syndromeIntersection syndrome is a painful condition that affects the thumb side of the forearm when inflammation occurs at the intersection of the muscle bellies of the abductor pollicis longus and extensor pollicis brevis cross over the extensor carpi radialis longus and the extensor carpi radialis brevis...
—pain will be more towards the middle of the back of the forearm and about 2–3 inches below the wrist - Wartenberg's syndromeCheiralgia parestheticaCheiralgia paresthetica is a neuropathy of the hand generally caused by compression or trauma to the superficial branch of the radial nerve. The area affected is typically on the back or side of the hand at the base of the thumb, near the anatomical snuffbox, but may extend up the back of the thumb...
Treatment
The management of De Quervain’s disease is determined more by convention than scientific data. From the original description of the illness in 1895 until the first description of corticosteroid injection by Jarrod Ismond in 1955, it appears that the only treatment offered was surgery. Since approximately 1972 the prevailing opinion has been that of McKenzie (1972) who suggested that corticosteroid injection was the first line of treatment and surgery should be reserved for unsuccessful injections. However, data regarding the efficacy of corticosteroid injection is sparse and uncontrolled (Oxford Level of Evidence 4) and it is not clear that there is a benefit over the natural history of the illness. A structured review published in 2003 identified only 35 publications that addressed De Quervain’s on Medline, only 7 of which presented data regarding corticosteroid injection, and none of which were controlled studies.Retrospective studies all report success rates for corticosteroid injection greater than 70%, but the one prospective cohort study noted a success rate of only 58% and many of those patients took 12 to 18 months until symptom resolution. While the authors of that study ascribed the failure of corticosteroid injection to anatomical variations, it has not been clearly established that corticosteroid injection is better than placebo or that a symptom course of 12 to 18 months is any better than the natural course of the illness.
Another commonly used criterion for failure of non-operative treatment is election of operative treatment, but the decision to operate is complex and biased by the beliefs and emotions of the surgeon and the patient. Use of an elective event such as surgery to define success makes data regarding nonoperative treatment difficult to interpret. For instance, in one of the two investigations in which a substantial number of patients were treated without injection (splints and anti-inflammatory medication alone were used), a remarkable 45 of 93 (48%) of patients in all non-operative treatment groups had surgery. This may simply reflect frustration on the part of both the patient and the surgeon with the prolonged symptom course associated with the disease. It may appear to both patient and surgeon that, after many months of symptoms, the illness will never resolve. The data of Lane and colleagues indicating that non-operative treatment is successful only in mild cases is similarly marred by the lack of patients randomly assigned to alternative treatments and the use in many patients of a decision for surgery as a failure criterion.
Most tendinoses are self-limiting and the same is likely to be true of de Quervain's although further study is needed. One retrospective series documented resolution in 90% of patients within 1 year
Palliative treatments include a splint that immobilized the wrist and the thumb to the interphalangeal joint and anti-inflammatory medication or acetaminophen.
Surgery (in which the sheath of the first dorsal compartment is opened longitudinally) is documented to provide relief in most patients. The most important risk is to the radial sensory nerve.
Physical/Occupational Therapy often focuses on lifting mechanics even though there is no evidence that activity modification can alter the course of the illness. Therapists can help fashion a splint that provides relief of symptoms by immobilizing the wrist and thumb. Splints have not been demonstrated to change the course of the illness.